Life Functions Critical
ECG-Sensors in cars, nano probes or epidermal electronics suitable for identification and for monitoring as well as surveilling life functions, are vital parts of the so-called Body Area Networks (BAN), an array of devices and sensors computing and transmitting body functions and health conditions by being implanted into or attached to the body. This chapter provides a media-archaeological approach to the technical and tele-medical arrangements of fictional, past, contemporary and future Body Area Networks to explain how the living body became a medium for data production and data transfer not only suitable for techniques of surveillance in a possible “ubiquitous cardiology”, but also producing new concepts of life and living in a growing data culture.
With Kubrick’s 2001: A Space Odyssey (USA/GB 1968), the optical and acoustic signaling of life functions being critical became iconic. The movie’s audience witnessed a spaceship’s computer killing the crew through seeing curves turn into flat lines. The same year, the Ad Hoc Committee of the Harvard Medical School published “A Definition of Irreversible Coma as a new criterion for death” (1968), shortly after the first transplantation of a human heart on December 3rd 1967 and amidst the so called “race to space”. Though there were some fatal losses in space flight in 1967, the audience of 2001 was ready to accept this sort of mediated statement about the difference between life and death. Nevertheless, relying on HAL 9000 as the supervising computer, the ambient assistant living environment every spaceship provides for human space travel turned into an ambient assisted death.

[Figure 1] Flatline Symposium (Source: 2001: A Space Odyssey 00:40:06)
Travelling through any kind of space has always raised questions about what is needed to protect the traveler and ensure a safe journey, producing and ceaselessly re-arranging — and therefore re-mediating — spheres of activity, of strangeness or wilderness, of homes or habitats, of hosts or threats, of crossing borders, secure arrivals and of what seems to be a precarious life.
However, with “life” being “a rather nebulous concept with extensive metaphysical connotations”, as Joanna Zylinska (2009, 65) puts it, the notion of “life” is an object of concern throughout a wide range of disciplines and politics. Therefore, the datafication of “life-functions” has become pivotal for discourses around care and concern, surveillance and protection, optimization and the preservation of human modes of existence. Bodies and life functions are turned into measurable, quantifiable, representable and therefore mediated data-products. This requires an assembly of medical-technical sensors and devices, which in turn require remote access to the body but also enable the body to be experienced in a different way. Living bodies and datafied bodies face each other in order to mediate life as a technological condition.
In 1968, the year 2001: A Space Odyssey was released, Soviet Professor of Biosciences and head of the laboratory of Physiological Cybernetics Pavel Guljaev suggested the polyclinic of the future:
A patient comes into surgery. The apparatuses record the electro-auragramm of his brain, his heart, his nerves, his muscles and viscera and send the information detected to an electronic diagnostic device, that, after calculating the disease, assigns the appropriate treatment. All this happens in a few seconds, the patient does not even have to take off his clothes (Guljaev 1968, 19).
Half a century after Guljaev’s and Kubrick’s visionary depiction of monitoring life functions, a watchOS update delivered a widely noticed EKG-functionality for the Apple Watch 4 to European users, a feature promoted as helping to save lives, supported by “real stories” of people that testify to how their “Apple Watch has become an indispensable part of their lives“ (Apple, 2018). Far from being a medical instrument but having at least the ability to monitor the heart and to produce warnings of what might be a critical state (e.g. atrial fibrillation) the declaration by Apple of the Watch as an “indispensable“ part of living reveals not only a sales strategy but the notion of technological tools becoming vital for the survival of their user, whether fit or unfit, carrying it anytime and everywhere.
Interested in the underlying concepts and conditions that link the named visions of a medical future and contemporary consumer products, this chapter investigates the media and technologies of datafication of so-called life-functions to explore the transitions related to human bodies travelling through digitized spheres of activity. Starting from historical and contemporary settings of monitoring life functions, it explains applications, concepts, preconditions and the biopolitical impact of a so-called ubiquitous cardiology together with the modes and techniques necessary for accessing bodies and life functions remotely via body area and sensor networks.
Monitoring the Heart’s Activity
In his 1891 textbook Augustus Desiré Waller presented the ”mode of distribution“ of variations of the electrical potential of the human heart in the form of a diagram, where the heart appears as the center of an electrical field that permeates the body.
Since the electrical activity of the heart can be “studied upon intact animals“, as he puts it, by “simply ‘leading off‘ from various points of the surface“ (loc. cit.), it is no longer necessary to expose the heart and attach electrodes to the heart itself.
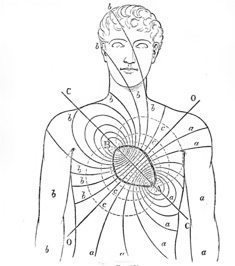
[Figure 2] Electric Heart (Source: Waller 1891, p. 388)
Following Waller’s concept, in 1907 the cardiac activity of patients at the Leyden hospital was wired via telephone into Willem Einthoven’s laboratory, where it was transformed into the shadow of the amplified movement of a string in the magnetic field of a string galvanometer and stored on photographic film. The patient at the hospital, sitting on a chair, their hands dipped in jars filled with sodium chloride, had no image of the machine he was connected with. Even though it is the action of the beating muscle inside their chest that matters, there is no direct materialization of the data recorded — the heart seems to be monitored without a monitor. Or, maybe by a distant monitor, as Fritz Kahn, famous for popularizing knowledge about the human body, demonstrated in his envisioning of “the doctor of the future“, who is supervising a patient traveling on a ship far out in the ocean (Kahn 1939, 198).
It is not only the ship in the ocean and its comparative, the spaceship, that suggest a fragile, precarious human life, with its life functions being endangered when travelling far out of reach of immediate or comprehensive medical support. Consequently, and according to the medical expansion of so-called danger zones in the 21st century, everyone is at risk, traveling through all kinds of spaces, even though some people may be more at risk than others and therefore considered to be a risk for others, too. The expansion of the risk-sphere itself is part of what, in Deleuzian terms, can be described as a “society of control”, where “the conception of a control mechanism, giving the position of any element within an open environment at any given instant” informs a “new medicine ‘without doctor or patient’ that singles out potential sick people and subjects at risk“ (Deleuze 1992, 7).
Hearts at the Wheel
At the end of March 2019, the European Commission announced that by 2022, safety technologies like drowsiness and attention detection, distraction prevention, intelligent speed assistance, vulnerable road user detection, reversing safety with camera or sensors, and event data recorders “will become mandatory in European vehicles“ (European Commission 2019).
But these technologies are not only related to other vehicles, pedestrians or cyclists, they also establish a constant record of the car’s occupants, monitoring their state of health as well as their use of technology and their ability to do so. The car might not start according to the level of blood-alcohol measured or it might stop according to an alarming state of glucose level or a cardiac episode. The detection of a severe cardiac crisis can initiate the vehicle’s assistance systems like lane assist, tempo limiter and emergency brake to intervene before the driver loses control. The system triggers a warning, stops automatically and calls for an ambulance, guiding it to the vehicle while constantly transmitting vital signs of its driver to a telemedics operation center.
Because the sensor-augmented technical ensemble of the vehicle configures itself as an activity sphere equipped with sign and road user recognition, distance meters and emergency braking, the “driver” can be dispensed of driving to become a “user”. “You can experience the car as a working world, as an entertainment world or as a rest area”, states Elmar Frickenstein (BMW 2019), former head of BMW’s Driver Assistance and Autonomous Driving Division with regard to what BMW calls Personal CoPilot. The option to pilot the car (i.e. to handle the steering wheel) remains, but it is one of many ways of using the car, which is called boost-mode by BMW (ibid.). The optional pilot-passenger no longer holds the key but is identified by the vehicle, for example, by checking biometrics such as face-recognition, fingerprints or the individual and unforgeable heartbeat, “identifying who you are and how you are“ (Goode Intelligence 2017). The data assessment of one’s individual heartbeat, a feature already predicted by Fritz Kahn to identify criminal subjects, nowadays becomes suitable for protecting and personalizing your car, starting the engine, authorizing in-car payments and supporting black box telematics as demanded by the EC, insurance companies (Allianz 2017) as well as law enforcement.
The transition from driver to user indicates a change of the dispositive. The driver now represents a vulnerable, sensitive, affect-controlled “interior” of the vehicle, a foreign body to be assimilated, whose intentions, affects and malfunctions must be analyzed and controlled in a similar way to the monitoring of tyre pressure or braking functionality. The driver has to be controlled, whereas the user has to be protected. Monitoring his life functions, the vehicle might become a diagnostic center that aggregates and processes a body knowledge far beyond the body knowledge of the user-driver themself, so that “time spent behind the wheel could possibly save drivers a visit to the doctor for a routine heart check-up” (Ford 2012).
Visiting a Guljaev-like diagnostic unit or clinic is not necessary, because a monitoring of cardiac functionality is possible as part of an ambient sensor network (ASN) that can be extended to mobile activity spheres. It is therefore sufficient to wear a watch or take a seat in your car. Just as imagined in Guljaev’s draft, it is not necessary to take off any clothes. As a result, the driver might get a call from the vehicle manufacturer or insurance company advising that they consult a doctor or even be directly contacted by their doctor about previously unknown heart problems. Heartbeat-derived data also delivers relevant information for establishing the parameters of control by the driver, which is of interest to car insurers for estimating risks and calculating insurance rates. Ford cites an up to 52% increased risk for cardiac patients of being involved in an accident (Ford 2012). Vehicle manufacturers, banks, financial service providers, mobile service providers, health insurance companies and transport authorities all take an interest in the mitigation of this increased risk. Therefore, organic bodily functions as well as cognitive abilities and affective states are being integrated into the sphere of data-processed locomotion and interconnected into dynamic interaction with other technical mobile activity spheres. The analytical vehicle thereby becomes a biopolitical instrument of prevention and risk minimization where constant monitoring would, for example, be the price for individual mobility in spite of conspicuous heart activity.
Subscribing to SuSes Sensory Surveillance System
The premise for a permanent and ubiquitous monitoring of the heartbeat seems to be obvious: “Bad heart always under permanent qualified observation, and every patient never without help – irrespective of moment of time and place on earth” (Augustyniak and Tadeusiewicz 2009: 1). Three elements are required for this: mobile and close-to-body sensory equipment, a wireless infrastructure and a hierarchical structure of analytical systems. At all these levels, the heartbeat configured as a vital sign is virtualized into a continuous stream of data. Usually, a cardiac sensation can be analyzed by those affected or by the environment within a matrix of symptoms related to behavior or signs indicating an emergency. But within mobile activity spheres a stabilization of this diagnosis is not readily possible. The extension of the danger zone therefore corresponds to the biopolitical measure of what Augustyniak and Tadeusiewicz call a ubiquitous cardiology, because “your heart is with you always and everywhere“ (ibid., 3).
According to Augustyniak and Tadeusiewicz, a ubiquitous cardiology can be implemented by subscription to web-based service providers of a “distributed surveillance system” (ibid., 228ff). This is controlled by a so-called Supervising Server (SuSe) that manages not only the electronic event recorder and thus the individual’s medical history, but also a variety of medical histories and medical data to deliver recommendations or treatment parameters based on a combination of artificial intelligence and efficient search algorithms. This requires a consistent self-monitoring routine of the technical systems to avoid malfunction or faulty signals, so that it is only in case of emergency that recourse must be made to medical expertise or medical intervention. In order to keep the amount of data low, as much data as possible should first be regulated at the level of the mobile devices. A device required for everyday monitoring could be cheaply distributed, borrowed, or integrated into existing technical systems, as shown by the example of a car seat, a steering wheel, a watch or a wristband. These systems are currently being developed as add-on devices combined with smartphone applications, whose computational and communicative capacities are being used just as Einthoven’s telephone network was between laboratory and hospital. The service will then include assurance of signal quality and artifact exclusion, computer-aided interpretation of the data, and medical intervention in the case of conspicuous cardiac events, that lead to either confirmation or correction of the machine’s interpretation, a patient recall, or advice provided for rescue services. But only a distress signal would change the priorities of the SuSe and ask for computer capacity. Nevertheless, the conception of such a system relies on a human backup in which at the end of the algorithmic routine there still is a medically trained operator or a tele-doctor on call — similar to Kahn’s doctor of the future.
Within distributed networks, the diagnostic algorithms implemented into the sensory devices are supplemented by network-based forwarding to increasingly specialized expert systems (ibid., 153;234-235). Therefore, priority features have to be set so that not all data has to pass all possible interpretive processes. However, increasing storage possibilities allow data aggregation and the implementation of additional parameters. Thus, the data not only aims at direct interventions but can be accumulated and used for making and marking a difference. It then produces a value per se, triggering various processes of normalization and relevance labeling, because the proposed subscription to a technology based service like this generates a multiple commitment strategy in which the monitoring of the current health status, as in the case of an automotive diagnostic unit, is transferred into an unknown knowledge of the body and a knowledgeable unknown about an interventionist risk management.
The diagnostic information a Guljaevian apparatus could provide would at best only be “a snapshot in time” (Yang et al. 2014, 6). But without continuous monitoring, finding “episodes” for Yang is a waste of time (ibid., 15). Yang et al. therefore suggest that continuous monitoring in the hospital should also provide information about the organizational and diagnostic procedures and processes: “Furthermore, in order to improve the efficiency of hospital systems, the movements of patients through its wards, clinics, emergency departments and operating theaters may be tracked to try and understand where workflow is being disrupted and may be streamlined” (ibid.,11). Therefore, the accumulation of data already is a mediated process of generating meaning and thus productive of itself. As this media-accumulation and the associated labeling of differences become algorithmized, it no longer relies on concrete intentions with respect to isolated data events, which then are nothing but special cases within a variability. These might trigger interventions or biopolitical decisions, but not as much as the aggregation and correlation of data always ready does. Ubiquitous cardiology then generates a technological ecology as an ensemble of lifestyle monitoring sensors and devices where cardiac monitoring as augmented cardiology is short-circuited with an augmented living as a real-time-based processing of an augmented reality. This digitally augmented reality conceptualizes body-space-relations beyond enhancement, prosthesis or simply implanted devices as activity spheres related to brains, hearts, bodies and movement, where everyone is at risk. Therefore, everyone becomes a user of supervising technologies that emerge from a pan-optical to a pan-sensual and then pan-informational monitoring of living as an activity sphere within networked spheres of activity, starting by carrying Apple Watches or using a car.
Sensors of the Body Area Network
For life functions to be monitored it is critical to integrate sensory ensembles into their technical and biological milieus. The visual or acoustic feedback strategies of mobile devices and their surfaces mask the tacit trust in the algorithmic processes of the SuSe and the subsequent medical interventions. For example, Augustyniak and Tadeusiewicz emphasize that SuSe center physicians interpret data from selected data events, treating patients based on data representations that are not negotiable for the implemented routines of the mobile device or the supervising server itself. However, this undermines one of the basic principles of emergency or intensive care medicine: to treat the patient rather than the monitor. As Didier Sicard points out, it is a medicine without a body — and thus possibly without an ethical subject (Sicard 2011, 417) — not far from the human bodies already consumed by their technosarcophagi on their space odyssey in Kubrick’s film.
Portable and mobile sensor technology requires so-called body area networks (BAN), that are an economic and normative setting of frequency bands, protocols, and routines, such as the IEEE 802.15.6 specification, agreed upon in spring 2012. The body is “a bag of water that does nasty things to channel models,” says Bob Heile, spokesman for the IEEE 802.15 Working Group on Wireless Personal Area Networks (Merritt 2012). In fact, the conductivity not only of body tissue but also of body fluids and gases plays a crucial role in the sensory measurement, for example by magnetically induced vortex fields (Steffen and Leonhardt 2008, 71). Thus the “human water bag” is not only relevant for the specifications of transmitting and receiving channels but contributes to the technological elements that become active on and in the body.
In contrast to neural activity, the shape and amplitude of cardiac activities as well as the discrete-time course are relatively constant. As shown above, the surging heart provides a continuous stream of data that provides information about whereabouts, mood, physical fitness and identity. Similarly, currents and electric fields vary in space and time as well as in intensity. Information can therefore be encoded via a spatio-temporal position within a medium. Digital techniques, on the other hand, use clock rates to quantify discrete intensities so that digital data representation allows filtering techniques and redundancies that can secure signal qualities while losing data in analog transmission mode. Nevertheless, analogue processing of body data is much more efficient, since it does not have to rely on a logic whose use in digital technology requires a multiplication of switching states, devices, or protocols (Shepherd et al., 2014, 276). In Body Sensor Networks (BSN), therefore, it makes sense to work with hybrid technologies, so that as far as possible, asynchronous digital techniques are used. This means that in the architecture of the electronic elements the division into an analog and a digital domain is considered (ibid., 281). In hybrid systems, at least the sensors themselves and their interfaces are analogous. Analog signal processing can be used very effectively for ECG frequency ranges. However, it is also possible to integrate analog data processing there, which is then passed on to digital data processing via an A/D converter. But how is the data transferred?
Hybrid chip designs integrate an electrode for a so-called human body communication (HBC). This means that the BSN is connected to the BAN via the body itself. For this purpose, the human body is used as a data transmission medium, because a wired network can indeed provide high data rates and a high signal-to-noise ratio, but is uncomfortable and prone to line interference. Wireless communication, on the other hand, is susceptible to transmission errors. Now, if the body itself can be used for signal transmission, both a high signal-to-noise ratio and high data rates are possible, while reducing the transceivers and the energy requirements. When the body itself is used as a data transmission medium by an implanted or body-worn sensor to possibly cause interventions placed on or in the body like drug delivery or electrical stimulation, the medialities coupled therein are folded one into one another: the body being both channel and receiver. Communication via an HBC allows interconnection with external data transmitters or integration into Guljaev-like scenarios, whereby a transmitting device is ensured by capacitive coupling with a body-near electrode and a receiving device by parasitic coupling with the surrounding environment (Wang 2014, 485). In capacitive coupling, the ground electrodes for data transmission need not be attached to the body because the electric field can be used for this. But in each case, grounding or the return channel is required over the environment. Body and environment therefore interact as a transport medium. This method provides high data rates of up to 10 Mbps with low power consumption, but may be susceptible to interference due to environmental coupling. Another version of HBC therefore is a so-called galvanic coupling. In this case, electrodes are attached to the body and, instead of the electric field, the flow of ions within the body is used as a waveguide. The disadvantage is a lower data throughput rate and the electrodes that have to be worn on the body. In both systems, surface-mounted sensors can be used as well as implanted or subcutaneous sensors or a sensory pill (Kiourti, Psthas and Nikita 2014). The parasitic biosensors use body tissues and body fluids for self-activation and travel through the body. Galvanic coupling is used to relay a time signal to a portable patch, which in turn can contact a smartphone and doctors or nurses to facilitate a digitized medication regimen.
Whereas traditional systems of multisensory vital signs monitoring are “poorly suited for practical applications outside of clinical research labs or settings” (Kim et al. 2011, 838) the devices of a ubiquitous cardiology are worn on or in the body, wired to or carried with the body. But the “wearables” can also become part of the body. As portable devices such as watches or wristbands used for mobile monitoring and sharing of vital parameters are already suited for daily use, further development of this might be an Epidermal Electronic System (EES).
While close-to-body or body-touching sensor systems are uncomfortable and irritating to the skin, epidermal electronics assemble what can be called an elementarium of sensor technology such as temperature sensors and electrophysiological sensors for EKG and EMG leads on an elastic polyvinyl alcohol layer. After washing out the PVA film, the Van der Waals forces are sufficient to form flexible “skin-like” membranes that conformally laminate onto the surface of the skin by soft contact, in a manner that is mechanically invisible to the user, much like a temporary transfer tattoo“ (loc. cit.). These so-called “transient electronics” dissolve after a while (Illinois 1867, 2012).
The technoskin can be applied to different parts of the body: at the throat to record verbal computer commands, on the forehead to monitor sleep, on the chest for reading cardiac activity. Although epidermal electronics can accommodate various sensors, it must be secured against elastic deformation energies when applied to the skin. While conventional silicon wafers are not flexible, the flexibility required for organic application can be achieved by reducing the thickness of the silicon layer. One way to accomplish this is to place electronic elements in a silicon layer and connect them to filamentary serpentine interconnects (Kim et al. 2011, 840). Another possibility are wave-shaped semiconductor nanomembranes that form a kind of herringbone pattern (Choi et al. 2007, 1655-1663). With the French personal care company L’Oréal presenting a wearable sensor to measure ph-levels of skin in January 2019, technologies like these are already on the verge of becoming consumer products.
Transitions of Transient Life
The sensory capacities of a so-called BAN and its wireless networking are constantly updating and exceeding thresholds. As they are no longer dependent on any graphic registration or imaging, which are nothing but special cases of data representation, the memory processes are media-accumulations and aggregations of states, events and manifestations as well as of the macro or micro differences between them. They do not configure the sensory or the sensible per se (Hansen 2011, 408-409) but the transition into an extended border regime that includes remote servers as well as the nanoprobe drifting through the bloodstream, the biometric car as well as wristbands, watches and technoskin.
As shown in this chapter, the Body Area and Sensor Network not only consists of sensorially augmented techno spheres of activity, but diffuse on to the body and under the skin, at the same time erasing borders and extending areas of control and intervention, defining critical life-functions and therefore life as always precarious.
The overlapping control systems form an infrastructure of control that operates in the gaps and below perception, a variable border regime of bodies, places, times, and liveliness that can be misunderstood as a new subjectivity and therefore be instrumentalized or reduced to users of a ubiquitous infrastructure of activity spheres where the body becomes its own active assisted ambient living. However, every algo-rhythmicity (Miyazaki 2013) of the body area network must be opposed to the obscure data acquisition in which a bodily life seems to disappear. But while life-threatening aspects of a computer malfunction, for example of autonomous vehicles, are still in discussion, HAL 9000 responds to the question of whether he bothers about the dependency on humans: “not the slightest BIT.“ (2001: 01:02:19)
Why should he?
References
A Definition of Irreversible Coma: Report of the Ad Hoc Committee of the Harvard Medical School to Examine the Definition of Brain Death. JAMA. 1968;205(6): 337–340.
Allianz. 2019. A brave new world: Vehicle Biometrics. Accessed April 15, 2019: https://www.allianzebroker.co.uk/content/allianzebroker/en_gb/application/content/documents/news-and-insight/industry/a-brave-new-world-vehicle-biometrics.current.html
Apple: Apple Watch — Real Stories — Apple. 2018. Youtube. Published 06.12.2018. Accessed April 15, 2019. https://www.youtube.com/watch?v=0tqB4jnCxqA&
Augustyniak, Piotr and Ryszard Tadeusiewicz. 2009: Ubiquitous Cardiology. Emerging Wireless Telemedical Applications. Hershey/New York: Medical Information Science Reference.
Bischofsberger, Catherine. 2017. “Wear your health on your sleeve.“ e-tech 05/2017. Accessed January 15, 2018. https://iecetech.org/index.php/issue/2017-05
BMW. 2019. BMW Personal Copilot: Autonomes Fahren. Accessed April 15, 2019: https://www.bmw.de/de/topics/faszination-bmw/bmw-autonomes-fahren.html
Choi, Won Mook et al. 2007. Biaxially Stretchable “Wavy” Silicon Nanomembranes. Nano Letters 7 (6): 1655–1663.
Dagdeviren, Canan et al. 2014. Conformal piezoelectric energy harvesting and storage from motions of the heart, lung, and diaphragm. In: Proceedings of the National Academy of Sciences of the United States of America 111 (5): 1927–1932.
Deleuze, Gilles. 1992. “Postscript on the Societies of Control.“ October 59.: 3-7, Cambridge: MIT-Press.
European Commission. 2019.: Road safety: Commission welcomes agreement on new EU rules to help save lives. Press Release. Accessed April 15, 2019: http://europa.eu/rapid/press-release_IP-19-1793_en.htm
Ford. 2012. The Ford heart rate monitoring seat. Ford ECG Seat Fact Sheet 05.2011. Accessed April 15, 2018. http://www.medtees.com/content/ecg_seat_fact_sheet_2.pdf
Goode Intelligence. 2017. Biometrics for the Connected Car. White Paper. Accessed April 15, 2019: https://www.goodeintelligence.com/wp-content/uploads/2017/11/Goode-Intelligence-White-Paper-Biometrics-for-the-Connected-Car-Identifying-who-you-are-and-how-you-are.pdf
Guljaev, Pavel. 1968. “Biologicheskaya svyaz’ deystvuyet.” Tekhnika Molodezhi, 12: 18-19.
Hansen, Mark B. N.. 2011. Medien des 21. Jahrhunderts, technisches Empfinden und unsere originäre Umweltbedingung. In: Die technologische Bedingung. Beiträge zur Beschreibung der technischen Welt. Edited by Erich Hörl, 365-409. Berlin: Suhrkamp.
Illinois 1867. 2012. Transient Electronics: UI Researcher Demonstrates Dissolvable Electronics. YouTube. Accessed April 15, 2019. https://www.youtube.com/watch?v=NnmHZXvJhlk
Kahn, Fritz. 1939. Der Mensch gesund und krank. Vol. 1. Rüschlikon/Zürich: Albert Müller.
Kim, Dae-Hyeong et al.. 2011. Epidermal Electronics. In: Science 333: 838-843.
Kiourti, Asimina, Konstantinos A Psathas and Konstantina S. Nikita. 2014. Implantable and Ingestible Medical Devices With Wireless Telemetry Functionalities: A Review of Current Status and Challenges. Bioelectromagnetics 35: 1-15.
Merritt, Rick. 2012. IEEE Group defines body area network. EETimes May 21, 2012. Accessed April 15, 2019. https://www.eetimes.com/document.asp?doc_id=1261777
Miyazaki, Shintaro. 2013. Algorhytmisiert. Eine Medienarchäologie digitaler Signale und (un)erhörter Zeiteffekte. Berlin: Kulturverlag Kadmos.
Shepherd, Leila, Timothy G. Constandinou and Christ Toumazou. 2014. Towards Ultra-low Power Bio-inspired Processing. In: Body sensor Networks. Edited by Guang-Zhong Yang. London: Springer: 273-29.
Sicard, Didier. 2011. De la médecine sans corps et sans sujet à l’éthique. In: Aux Origines de la Médecine. Edited by Georges Vigarello and Didier Sicard, 417-429. Paris: fayard.
Steffen, M. and S. Leonhardt. 2008. Non-Contact Monitoring of Heart and Lung Activity by Magnetic Induction Measurement. Acta Polytechnica 48 (3): 71-78.
Waller, Augustus D. 1891. An Introduction to Human Physiology. London: Longman, Greene and Co.
Wang, Lei et. al. 2014. Wireless Sensor Microsystem Design: A Practical Perspektive. In: Body sensor Networks. Edited by Guang-Zhong Yang, 463-494. London: Springer.
Yang, Guand-Zhong et al.. 2014. Introduction. In: Body sensor Networks. Edited by Guang-Zhong Yang. London: Springer: 1-53.
Zylinska, Joanna. 2009. Bioethics in the Age of New Media. Cambridge, London: MIT-Press.
2001: A Space Odyssey, USA/UK 1968, R: Stanley Kubrick, D: Stanley Kubrick und Arthur C. Clarke.